
I Was Hospitalized - 074

Before I tell you about my hospitalization, I need to tell you about my latest lab results.
On March 5, 2026, a comprehensive set of labs was normal except for a PSA of 640 ng/mL, a significant increase from my prior PSA of 395.90 ng/mL on October 28, 2025.
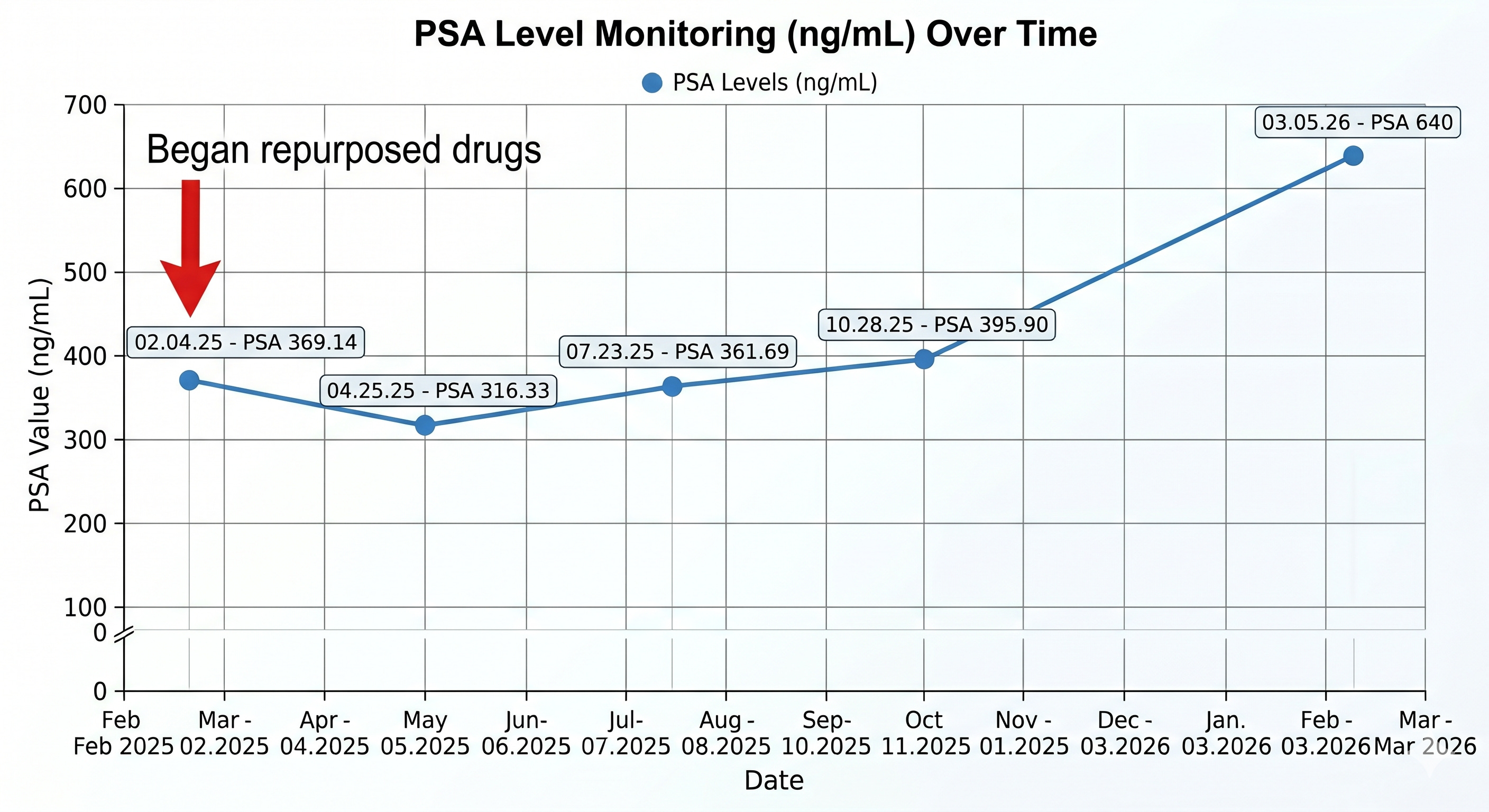
The graph shows my PSA values since starting Ivermectin, Fenbendazole, and Methylene Blue. My PSA initially dropped by 53 points, then slowly started climbing again, but with a much longer doubling time than my previous 9-month doubling time.
So what happened between October 28, 2025, and March 5, 2026? A few things, but I’ll save those for the next newsletter as this one is pretty long.
That rising number was the background noise to everything that followed in this article - a constant, low-frequency hum of anxiety that I didn't realize was setting me up for a fall.
Let’s get back to my hospitalization.
How it started
I didn’t sleep well for two nights in a row beginning April 13, 2026, with a really terrible night on April 14, 2026, when I woke up at 1 AM and couldn’t fall back asleep.
Despite feeling exhausted, I went to work on April 15, arriving at my usual start time of 7 AM. We were super busy that day, and I barely had time to stop and drink water.
Around 11 AM, I was seeing a patient, stood up from my desk, and suddenly felt lightheaded. I raised my arms, but I had difficulty lifting my left arm.
My heart started racing, and the lightheadedness persisted. As soon as I realized that my left arm felt weaker than the right, I convinced myself I was having a stroke.
I sat down in my chair, regained my composure, and then slowly completed the visit. The lightheadedness persisted, and I no longer felt that my left arm was weak, but it felt heavy.
All I could think was, “I’m not going to be taken out of my office in a stretcher by emergency medical services. I let another physician know I wasn’t feeling well and walked out to my car, still feeling weak.
I called Mike and told him I thought I was having a stroke, and that he needed to come pick me up and bring me to the emergency room (ER). He told me to call 911, but I told him I’d wait until he got there.
B.E.F.A.S.T. - an acronym used to recognize the signs of a stroke
As I got to my car, I could feel my heart pounding. I did a quick “BEFAST” assessment: Balance, Eyes, Face, Arm (or Leg), Speech, Timing.
I stood on one leg, and that was okay. I raised my arms and held them out in front of me, and neither one drifted. I looked into the rearview mirror and smiled, looking for facial asymmetry - none.
I had kept Mike on the phone and asked him if my speech was okay. He said, yes. As for timing, everything was moving pretty quickly, and I knew I’d be getting to the ER soon.
Impending doom
Everything looked normal, but I had this feeling of impending doom. I kept Mike on the phone until he arrived, and then I got into his truck. I must have looked pale as a ghost because he said you don’t look good.
I told him which emergency room I wanted to go to, and we headed there. I was pretty sure the hospital was a certified stroke center, but I double-checked by looking it up on my phone.
As Mike was driving us there, I still had this heaviness in my left arm and started feeling a weird sensation in my left face. The impending doom was escalating, and I told him that if things went south, I didn’t want any heroic measures, no intubation.
His voice cracked, and he told me to stop talking like that.
I had this brief visualization of me sitting at my writing desk at home, paralyzed on my left side, and attempting to type with my right hand only. It’s so strange where your mind will take you in a stress response.
That’s when Mike put his right hand on my chest and started saying over and over, “You are safe, you are safe.” And he reminded me to do some deep breathing.
The emergency room
It wasn’t long before we pulled up to the ER, and he asked me if I was okay walking. I said yes, slowly got out of the car, and began walking to the entrance.
A security guard was at the entrance, and I told him I wasn’t feeling well. He walked me to the desk. I told the receptionist that I was a doctor and that I thought I might be having a TIA (transient ischemic attack) or a stroke.
She asked me why I thought that, and I told her that my left arm and the left side of my face felt heavy. She immediately called for a wheelchair and triggered her walkie-talkie, saying, “ A patient with numbness.”
Within a few seconds, I was in a wheelchair and rolling into the ER. They had me get up onto a gurney in the hallway, and the ER doctor came over, took a brief history, and performed a cursory neurologic exam.
She instructed the nurse to push my gurney into a trauma bay. My nurse established automatic blood pressure monitoring and automatic cardiac telemetry, attached a pulse oximeter to monitor my oxygen status, and inserted a heparin lock - an intravenous line capped with a port.
Someone else performed a fingerstick to check my blood sugar - it was 111. Then a tech arrived to take an electrocardiogram (ECG). I didn’t look at the telemetry monitor or see my ECG, but I’m sure it showed an elevated heart rate and blood pressure.
My ER nurse, who was absolutely fantastic and who performed neurologic testing on me every 10 minutes, asked Mike if my face always had a slight droop. He and I both answered yes, as I’ve always had a little facial asymmetry since a guy punched me in the jaw in college. But that’s another story.
The ER doctor returned, took a little more extensive history, and I could see she became very concerned when I told her my prostate cancer history. At that point, she added neurologic metastases to the differential diagnoses.
The ER doctor performed another cursory neurologic exam and asked me if I was feeling anything abnormal - pain or weakness? I told her my left arm still felt heavy and that I still had this weird sensation in my left face.
The stroke protocol begins
That’s when she called for the stroke protocol to begin in full force. She said something like, “I’m calling it,” as if everyone had already discussed it before entering my room. And as quickly as she entered the room, she was gone.
A funny thing I remember is Mike asking me if doctors still use stethoscopes, and I said, “I guess not.”
I was immediately wheeled to the imaging section and underwent a Head CT with and without contrast. I also underwent CT angiography of my head and neck.
I hadn’t received iodinated contrast in a while, and I was surprised by how intense the warm, tingling sensation in my core was as the tech injected it. The imaging tech wheeled me back into the ER, and after a few minutes, my nurse walked in and calmly started entering data into the computer.
At that point, I turned to Mike and said, “ I didn’t have a stroke, because if I did, they would already be administering the clot buster.” I was relieved.
Then, the ER physician walked in, confirmed that my Head CT was normal, and said, “The hospitalist ordered an MRI of your brain and cervical spine.” I thought that was strange since I hadn’t met the hospitalist yet.
Over an hour in the MRI machine
The nurse then wheeled me to the MRI section. The MRI tech kindly greeted me and asked me if I felt well enough to walk to the MRI machine. I answered, “Yes,” removed my glasses and belt, and emptied my pockets before lying down on the MRI bed.
She laid a warmed blanket over me and told me she would talk me through the imaging as we went along. She put earplugs in my ears, placed a plastic device around my head to keep me from moving, and padded the sides of my head so it was super snug.
She placed a button in my hand to press if I felt like we needed to stop, and off we went. I’m not a very big person - 5’10” and 168 lbs, but my shoulders are broad. It felt and looked like I was being squeezed into a tight white coffin.
The area above my eyes was approximately 5 inches from the ceiling of the MRI machine, and even with earplugs and padding next to my ears, I could hear the very loud, rhythmic pulsing of the machine as it progressed through the various stages.
I can totally understand why someone might have a panic attack in an MRI machine.
I was in the machine for about 20 minutes when I heard it spool down, and the sliding table underneath me moved out of the machine and back into the open.
I’m thinking, okay, that wasn’t too bad, when she walked up to me and said that she had additional orders. I was now going to get scanned again, this time, my brain (again) and cervical spine with and without an injection of gadolinium - a contrast agent that helps enhance the images.
Someone made a mistake, but I’m not complaining and just going with the flow. Back into the machine I went for imaging before and after the injection, this time without any warm, tingling sensation.
By the time it was all said and done, I had been in the MRI machine well over an hour. When the MRI bed slid out this time, I could feel an intense spasm in my left trapezius and the onset of a low-grade tension headache.
I have pretty significant degenerative changes in my cervical spine, known from previous scans. Because I didn’t have proper neck support during this very long MRI scanning, the positioning flared the underlying disease and caused my neck and upper back muscles to intensely spasm.
A potential cause for my symptoms
As I focused on the spasm in my left trapezius, I realized this was what was making my arm feel heavy and causing a tugging sensation in my left face. I had a sudden epiphany that the spasm had been there all along, and I hadn’t noticed it earlier because of my intense fatigue.
Could this be the root cause of my original symptoms? As I sat up on the side of the MRI bed, I lifted my left arm and felt a mild restriction. I still wasn’t convinced I hadn’t experienced a TIA or had neurologic symptoms from mets to my brain or spine.
The tech got me back up on the gurney and wheeled me back into my ER room. That’s when the nurse pointed out that I had a lot of blood on my dress shirt near the heparin lock. She immediately started saturating it with hydrogen peroxide, and I politely told her not to bother, since it was so extensive that I’d throw the shirt away.
She helped me take off my shirt and put me in a hospital gown, while I still wore my dress pants and dress shoes. Mike, who has previously passed out at the sight of blood, calmly picked up my shirt, folded it, and placed it in a clear plastic bag.
Wow! He is being so strong through all of this.
Good news and a whole body release
The nurse reattached the pulse ox, automatic blood pressure cuff, and telemetry monitor, and a few minutes later, the ER physician walked in and told us that the radiologist had looked at my MRI scans and said there is no evidence of stroke or metastases, but that the neuroradiologist still had to read them.
I thanked her, and she walked out. As soon as she walked out, my body began trembling. It was subtle but visible, and lasted about a minute. It was obvious enough that Mike came over and held my hand. As soon as the trembling stopped, I felt this dramatic relaxation come over my entire body and mind.
I had received the definitive news that I didn’t have a stroke and didn’t have evidence of neurologic metastases. I could finally start to relax.
It is comparable to an animal in the Serengeti escaping a predator, shaking its entire body, taking a deep breath, and going back to eating grass. It’s an attempt by the nervous system to reset so it doesn’t stay in fight-or-flight mode.
About 15 minutes later, the ER physician returned to tell me that the neuroradiologist had read the images and everything looked okay, but that the hospitalist wanted to keep me overnight for observation. I still had not seen the hospitalist.
The man behind the curtain
I thought it was strange that the hospitalist was making all these calls without having spoken to or examined me. I also found it strange that the ER physician had performed only a brief neurologic exam and no other components of a physical exam despite the numerous times she interacted with me.
Is that how medical evaluations in the ER and hospital admissions work these days? Have doctors become so overly reliant on technology that the physical exam has become an afterthought? My medical training wasn’t like that, but maybe medical training has changed.
Before the ER nurse wheeled me up to my room, I told her she did an excellent job and was very kind and compassionate. She thanked me with a big smile.
I was lying in my hospital bed when the hospitalist walked in and introduced himself. I had heard his name mentioned in the ER, looked him up on my phone, and saw that he was one year out of residency. He seemed nice.
The incidentaloma
He told me that my imaging showed that I have no evidence of ischemia or stroke, but that I do have a small pituitary microadenoma that shows up on my brain MRI but not the CT scan.
Whenever you image the body enough, especially with MRI scans capable of finding the smallest of things, you inevitably come across an ‘incidentaloma,’ defined as an asymptomatic mass or lesion discovered unexpectedly during diagnostic imaging or testing performed for an unrelated reason.
This finding was tiny and asymptomatic. If it were symptomatic, I’d have difficulty with my vision as it sits near where the optic nerves meet and cross over. In addition, if this were negatively impacting my downstream hormones, I wouldn’t have a normal thyroid panel and testosterone, which I do. And might even have lactating breasts if it causes prolactin levels to be high.
His recommendation parroted the neuroradiologist’s instructions to perform a dedicated pituitary MRI with cuts through the pituitary. In other words, repeat an MRI focusing on the pituitary. I’m opting to do this in one year since the incidentaloma is asymptomatic and very tiny.
Cervical disc disease and muscle spasm
He also told me I had multi-level degenerative disc disease of my cervical spine with several small disc herniations and several areas of neuroforaminal encroachment. Meaning several small disc herniations causing impingement on the nerve roots as they exit my cervical spine.
It’s no wonder I have this massive left upper trapezius muscle spasm. I told the hospitalist about this and asked if he thought it might be causing some of the symptoms I presented with, and he answered, “Yes, it’s possible.”
He asked me if I’d like to try a muscle relaxer to see if it would help, and I agreed. He added Robaxin, as needed, to my inpatient medication list.
Doctors’ exams aren’t like they used to be
He then performed his physical exam, which consisted of placing his stethoscope on both sides of my anterior chest. That was it. That was the hospitalist’s physical exam.
He did not perform even a cursory neurologic exam, did not assess my reported left trap spasm, did not listen to my carotids or posterior lung fields, did not listen for bruits in my abdominal arteries, did not check for peripheral edema, and did not check my peripheral pulses.
In fact, he didn’t even ask me to stand or walk, and he spent less than 10 minutes with me.
I guess I’m not surprised. When I underwent a radical prostatectomy in 2018, a hospitalist saw me for the first time the morning after my surgery, lifted my gown to look at my traumatized abdomen, never asked me about any personal or family history, didn’t lay a hand or a stethoscope on me and then documented in the medical record a comprehensive history and physical, which seemed to have been copied and pasted from a combination of my urologist’s and anesthesiologist’s notes.
I’ll be disappointed if that’s what I see when I request my hospital records. I know the documentation requirements have changed significantly since 2018, but do ER doctors and hospitalists perform very limited histories and physical exams these days? I’m just asking.
The nurses were amazing
Anyway, I sincerely appreciate the attentive care and thorough work-up. The nursing care was outstanding, and the very young certified nursing assistants (CNAs) were spot-on with their duties, coming into my room every 4 hours to take my vitals, even though I was on telemetry.
The nurse who admitted me to my room was young and very kind. She performed a thorough exam, including a detailed neurologic exam and a comprehensive physical exam. She and I hit it off, chatting about things medical.
About thirty minutes after the hospitalist left, the nurse brought me a Robaxin and an aspirin. Thank goodness, because there was no way I could sleep with this massive, tender muscle spasm in my left trapezius.
Then the shift change happened, and I was introduced to my next nurse, who was about my age, no-nonsense, but also very kind. I felt like I was in really good hands with these nurses. Another detailed exam, and my younger nurse told me she would see me in the morning.
Mike, who had been sitting in the chair by my bed, looked exhausted, and I told him I’d be in good hands and that he should go home and get some sleep. He kissed me goodbye and left.
By about 10 PM, I realized the Robaxin and aspirin didn’t do a thing for the muscle spasm, and I reluctantly buzzed the nurse and asked her if I could get some ibuprofen. She told me that it wasn’t on my list of medications and that she’d have to call the hospitalist to get an order.
Ibuprofen to the rescue
I said, “Yes, please do,” and she asked me what dose. I said, “600 mg, please.” Just after 11 PM, she arrived with the 600 mg ibuprofen, and I swallowed it immediately.
Within an hour, I felt the spasm start to melt away and felt relaxed enough to feel like I could sleep now. What’s telling is that as the spasm started to dissipate, the heaviness in my left arm and tugging sensation on my left face also resolved.
Just as I was falling asleep at 12 AM, the CNA walked in and performed vital signs. An hour later, the nurse arrived to replace all my leads on the telemetry monitor, as it had stopped working.
At 4 AM, the CNA promptly returned to take vitals. So, unfortunately, I didn’t get any sleep while I was in the hospital.
My nurse to the rescue
At 7 AM, the nurse who had admitted me to the floor the prior day arrived for duty and wished me good morning. She asked me if I was having any symptoms, and I said, “None at all.” She said, “Great, as soon as the hospitalist arrives, I’ll advocate for you getting discharged.’
She told me a neurology consult was scheduled for this morning, but it didn’t seem necessary given that all my tests and neurologic exams are normal, and that I have no symptoms.
I was so thankful to hear that, as I was very ready to go home.
About 10 AM, the hospitalist arrived and told me he had canceled my neurology consult and was about to write my discharge orders. He said that because all my labs, imaging, and current vital signs are normal, he was not discharging me on any new medication and that I should follow up with my primary care physician.
He let me view my labs on his smartphone, and I saw that my complete blood cell count, comprehensive metabolic panel (including liver enzymes), alkaline phosphatase (usually elevated with bone mets), and hemoglobin A1C (diabetes marker) were all normal.
My total cholesterol was 160, LDL 109, HDL 48, and triglycerides 66 - suggestive of low cardiac risk.
I thanked him and texted Mike to come and pick me up.
The neurologist drops by
I hear a knock at the door, and the neurologist walks in and introduces herself. She was young and very kind. She said, “Hi, I know your neurology consult was canceled, but I know you are a doctor, and I just wanted to introduce myself.”
We briefly discussed the testing, and I also described the muscle spasm in my left trapezius and how that could have played a role. She told me that I had significant neuroforaminal encroachment on my cervical spine MRI and that this could very well have been a TIA mimic.
A TIA mimic is a condition that produces temporary neurological symptoms similar to a “mini-stroke,” but is caused by non-vascular issues.
She told me that if the muscular spasm is severe enough to compress the nerves leading to my arm, it can cause paresthesia. I thanked her for stopping by and for her input, and she left.
My escape
My nurse walked me to the elevator, and as the elevator door opened, I saw Mike. I told the nurse that she did a fantastic job and thanked her. I joined Mike, and we left the hospital.
Thank God for nurses
And
Thank God for Mike, my precious earth angel
Then something strange happened. As we were walking across the parking lot to Mike’s truck, I started feeling the fear that I felt when I first got to the hospital.
Was I feeling fear because I was leaving the “safety” of the hospital? That’s what it seemed to me. Mike reassured me, and we drove home.
As soon as I walked into my home, the fear completely resolved, and I felt an energy shift. I thought, “My home feels really safe. I can relax again.”
That night, I slept the soundest I’ve slept in weeks.
In retrospect, putting all the pieces of the puzzle together, I feel this event was caused by sleep deprivation, mild dehydration, and the muscle spasm in my left trapezius.
And there’s the elephant in the room - an adrenergic surge, likely a panic attack caused by misinterpretation of my body’s sensations while severely fatigued, aggravated by the stress of seeing my PSA persistently rise, now 640, and waiting for the next shoe to drop.
Miraculously, and I don’t use that term lightly, despite a PSA of 640 ng/mL, I have no other signs or symptoms of metastatic prostate cancer, and all of my other labs and diagnostic testing are normal.
In the next newsletter, I’ll discuss the changes following my October labs that may have contributed to the more rapid increase in PSA, as well as the plan from here.
Give those you love a big hug and tell them you love them. You never know what’s around the corner.
Until then, I wish all of you good health and much love,
Keith
It is good to read that your symptoms were almost certainly not a stroke or TIA, as I’m sure you are. I’m a retired internist and geriatrician who practiced from 1979 until 2020, so I have seen lots of changes in the way medicine is practiced. For all of my career I practiced in New Jersey so all of my physicians were people I knew and who knew me. Now that I’ve moved to Connecticut and am seeing all new doctors they spend less time with me and the exams are often much more cursory that how I was trained or experienced. While advanced technology has helped make a diagnosis, the human aspects of providing care are lost when you know little about your patient and have barely put your hands on them. The trust a patient puts in their doctor still is an important part of healing. Best wished for continued good health despite the prostate cancer.
Dear Dr. Keith--long-ago, ashort-term pt of you in NE FL. Heck of a tale you told. Will look for your thoughts on the rising PSA. Plan to share this with my solo practice, former nurse turned physician, here in Orange Park. Carry on with life. And with Mike.