
I Had Such High Hopes for Pluvicto - 059

Remember the buzz? When Pluvicto (the catchy name for Lutetium-177 vipivotide tetraxetan, or 177Lu-PSMA-617) arrived on the scene in the United States (U.S.) with FDA approval in March 2022 to treat metastatic castrate-resistant prostate cancer (mCRPC).
Many in the U.S. hailed this targeted radioligand therapy as revolutionary, promising a new weapon in the fight against mCRPC.
Germany a step ahead of the U.S.
As is sometimes the case in medical therapies, the U.S. was several years behind Europe regarding PSMA radioligand therapy. Germany had widely adopted PSMA radioligand therapy for mCRPC as early as 2013 under a compassionate use program. Before its approval in the U.S. in 2022, some American men with mCRPC were traveling to Germany and paying cash for treatment.
In some instances, German physicians are also using it to treat metastatic castrate-sensitive prostate cancer (mCSPC), including men from the U.S. who pay cash for treatment. It is only FDA-approved for mCRPC, and no clinics in the U.S. are using it, outside of clinical trials, to treat mCSPC.
Prostate-specific membrane antigen (PSMA)
PSMA stands for prostate-specific membrane antigen, which is a misnomer. This protein also exists on the cell surface of other cancers and some healthy tissues, such as the salivary glands and small intestine. However, it is found on prostate cancer cells and not on healthy prostate cells.
Yes, its name makes things confusing. However, it is a reliable marker for prostate cancer cells in that 90% of prostate cancer cells, both CSPC and CRPC express it.
PSMA radioligand therapy is part of a theranostics system. The diagnostic part is the PSMA positron emission tomography (PET) scan, and the therapeutic part is the PSMA radioligand therapy (Pluvicto). The PSMA PET scan detects the expression of PSMA on prostate cancer cells, and Pluvicto treats it.
Precision radiation
Pluvicto is a precision type of radiation in which a radioisotope is injected into the bloodstream. The radioisotope then locates and binds to the PSMA antigen on the prostate cancer cell surface.
Once the radioisotope binds to the cell surface antigen, it releases a two-millimeter radiation burst, killing the tumor cell. It's such a small burst of radiation that it tends to spare healthy tissue, unlike typical radiation therapy.
However, despite such a small burst of radioactivity, collateral damage can occur to healthy tissue. Because the salivary glands express PSMA, their damage can result in a dry mouth, which is rarely severe and permanent.
Patients with extensive bone metastases, especially those with prior chemotherapy, can develop bone marrow suppression with low red blood cells (anemia), low platelets (thrombocytopenia), and low white blood cells (neutropenia).
Yet another example of how Germany outshines the U.S. is using prophylactic ice packs on the salivary glands to induce vasoconstriction, reducing blood flow and PSMA ligand uptake in the salivary glands, thereby lowering radiation exposure.
In Germany, a low-cost ice pack applied to the salivary glands during PSMA-radioligand therapy is the standard of care due to observational data and real-world evidence of its effectiveness.
Infuriatingly, most clinics in the U.S. don't bother using ice packs during treatment to prevent dry mouth. Why? Because no one in the U.S. has done a U.S. phase 3 clinical trial to prove it works. Ridiculous! Just look at the data from Germany.
So, if you are a patient in the U.S. getting Pluvicto, bring your own ice packs to help avoid getting dry mouth!
The VISION trial
Speaking of infuriating, let's discuss the phase 3 VISION trial that got Pluvicto approved in the U.S.
The study showed that Pluvicto when added to standard care, did indeed help men live longer than standard care alone. Success!
But here's where we need to put on our critical thinking caps.
What did "living longer" actually mean in the trial that paved the way for Pluvicto's approval? The VISION trial showed Pluvicto extended median overall survival by four months, meaning the midpoint of survival was extended—but this still reflects a grim prognosis for many participants.
Let me be clear. In the face of mCRPC, any extension of life is precious. For the men and families receiving that extra time, it's invaluable.
Pluvicto also demonstrated benefits in delaying disease progression and improving quality of life, which are hugely important. It represents real, tangible progress and a valuable addition to treatment options for mCRPC.
A critical look
But let's step back from the initial celebratory fireworks. Did a four-month median overall survival advantage live up to the 'game-changer' narrative often given to new therapies?
This isn't just about Pluvicto. It's about a broader pattern I see time and again in the development of treatments for heavily pre-treated men with mCRPC.
Honestly, achieving big leaps in survival at this late stage of the disease is incredibly difficult. By the time men qualified for the VISION trial, their cancer had already outsmarted multiple lines of therapy, including androgen deprivation therapy (ADT), potent androgen receptor pathway inhibitors (ARPIs), and taxane-based chemotherapy.
Their disease was, by definition, highly resistant. So, maybe the 'secret' isn't that Pluvicto's benefit was only four months, but rather that achieving even that much is a significant accomplishment in such a challenging setting.
The surprise might be less about the result and more about how it contrasts with the hope and hype often surrounding new drug approvals. Is it possible that we, as patients, physicians, and observers, sometimes set high expectations only to feel let down by the current reality of mCRPC research? I admit that I do.
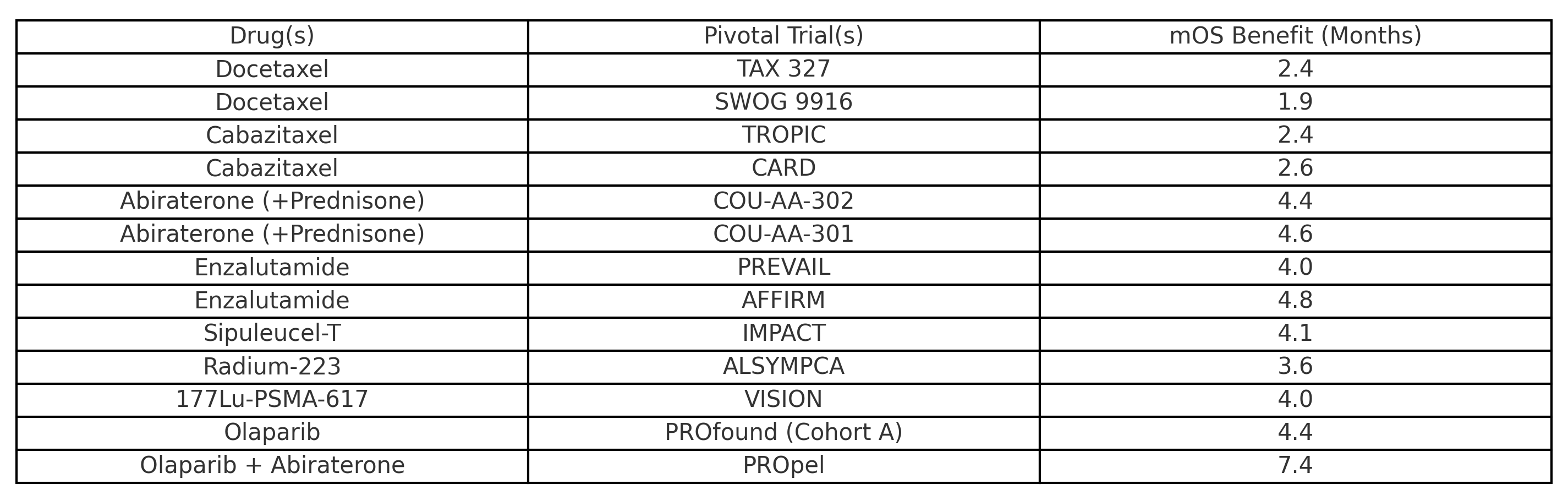
Looking at other therapies approved for mCRPC, you'll see a similar pattern - relatively low median overall survival benefits.
I still have high hopes for Pluvicto and am looking forward to seeing what it can do in clinical trials involving men with castrate-sensitive prostate cancer.
VISION’s unethical trial design
While I'm disappointed in the VISION trial's results, I'm very unhappy with its design. Here's why.
The VISION trial's control arm (standard-care therapies) was poorly designed and limited the use of pharmaceuticals with a survival benefit. In other words, it allowed suboptimal treatment options.
This was a disservice to the men in the control arm, who might otherwise have received the real standard of care outside this clinical trial. Some might say it was malpractice.
For example, 50% of men in the control arm were eligible for cabazitaxel, which showed a survival benefit over androgen receptor pathway inhibitors (ARPIs) in the CARD trial. But they couldn't get it because of the VISION trial rules.
Nor could men in the control arm with only bone metastases get systemic radioisotopes like radium-223, which has shown a median overall survival of 15 months.
In addition, 55% of men in the control group had already received one ARPI, and 39% had already received two. This significantly limits hormone therapy options in the control group because the clinical efficacy of switching one ARPI to another is not very good at all.
A control group should always get therapies that are the prevailing standard of care, and in the VISION trial, men in the control group did not receive the prevailing standard of care. That is unethical.
In addition, this phenomenon of a suboptimal control arm is widespread in pharmaceutical-sponsored clinical trials. Why? Poorly designed control arms that don't allow life-prolonging therapies potentially make the study (drug) look better than it is.
The VISION trial designers tried to rationalize excluding certain treatments by saying that the safety profile of these therapies had not been established with Lu-PSMA-617. However, that is no excuse for designating a terrible control arm. They could have allowed men in the control arm to receive cabazitaxel.
High rate of dropout in the control arm
If I were enrolled in a clinical trial that prevented me from taking a standard of care therapy that has the potential to prolong my life, I would be angry and drop out of the study. And that appears to have happened in the VISION trial.
After the trial started, the control group had an extremely high incidence of withdrawal—56%—mainly attributed to patient disappointment. This is an example of cutting off data too early in the control group, which messes up the trial results and makes later measurements less trustworthy.
When the trial designers saw this, they implemented “trial-site education measures” to reduce the incidence of withdrawal—basically, they convinced patients to stay in a poorly designed control arm. That is simply wrong.
I've discussed poorly designed clinical trials with suboptimal control arms before. Please read that Substack post if you haven't already done so. It is eye-opening.
Conclusion
Even modest survival gains are meaningful in clinical trials involving heavily pre-treated men with mCRPC. Still, these gains should not be overhyped or come at the cost of ethical compromise in trial design.
Men with mCRPC considering enrolling in a clinical trial should understand the importance of an ethical control arm. Even if you consult with a physician at a prostate cancer center of excellence, sometimes these physicians are biased, especially if their center participates in the clinical trial.
Until the next one, I hope you stay healthy.
Much love,
Keith
I haven’t reached the need of going to some exotic treatment like Pluvicto but I’m not sure that I would even if I had a need. As I understand it in Canada, the cost is not covered by Medicare and that means about a $200,000 bill for four treatments at $50,000 each which are necessary to save you an estimated two extra months of life.
where is the percentage in that🤷♂️
The method of how to prevent the dry mouth could be a game changer for some.
Instead i’m activating my stay healthy plan of taking 72mg of ivermectin daily along with curcumin capsules and pepper morning and night along with several cups of green tea each day.
My PSA after salvage radiation were rising steadily until the ivermectin plan came into place. Scores of.
0.01 to 0.02 to 0.03 in quick order have ended up stabilizing at 0.03. I will know the effectiveness of my plan in three months time when I have another PSA test.
Hi Keith, I've investigated radioligand treatments around the world. I've discussed the treatments with men who have chosen to pursue the care themselves in Austraila, India, Germany and Canada. The cost varies from $5K in India to free-for-all excessive pricing in Canada. The whole concept of clinical trials is ripe for conflict of interest whenever docs from COEs involve themselves with Pharma.
When countries with national healthcare begin using treatments that have not been pursued in the US and those treatments work well and inexpensively - think transdermal tE2 in the UK in place of Lupron for ADT - you know that the absense of a treatment use in the US is caused by there not being enough profit in the development of a treatment drug for Pharma to get involved. It continually pisses me off, but I know it is how the American medical system has been constructed. I don't have to lîke it.