
Genetic Breakthroughs in Prostate Cancer: Unlocking the Potential of PARP Inhibitors - 055

When diagnosed with advanced prostate cancer, patients may feel their options are limited. However, breakthroughs in genetic testing and targeted therapies like polyadenosine diphosphate - ADP -ribose - polymerase (PARP) inhibitors give patients new options. What if the key to treating your cancer lies in your deoxyribonucleic acid (DNA)?
Prostate cancers may exhibit abnormalities in DNA damage repair pathways. In the last newsletter, I discussed DNA repair genetic mutations that may respond favorably to immunotherapy, like the checkpoint inhibitor pembrolizumab (Keytruda).
In this newsletter, I show how prostate cancer that has a deficiency of a DNA repair pathway called homologous recombination repair (HRR) can be susceptible to drugs called PARP inhibitors.
PARP inhibitors approved for prostate cancer
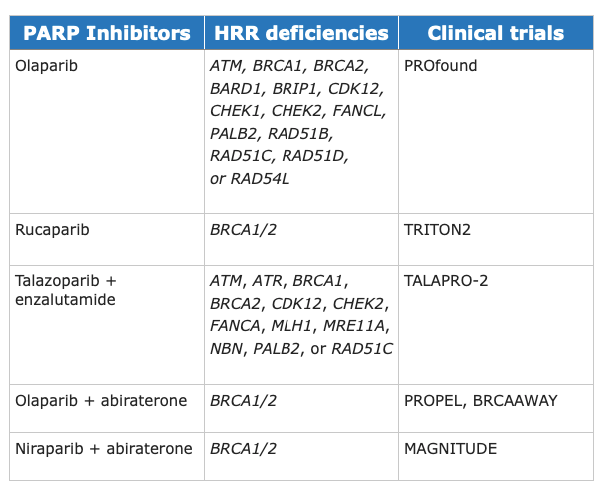
The following PARP inhibitors are approved for treating metastatic castrate-resistant prostate cancer (mCRPC) in men already on androgen deprivation therapy (ADT). Studies also show that enzalutamide (Xtandi) and abiraterone (Zytiga), combined with PARP inhibitors, are effective against specific HRR mutations.
Mechanism of action of PARP inhibitors
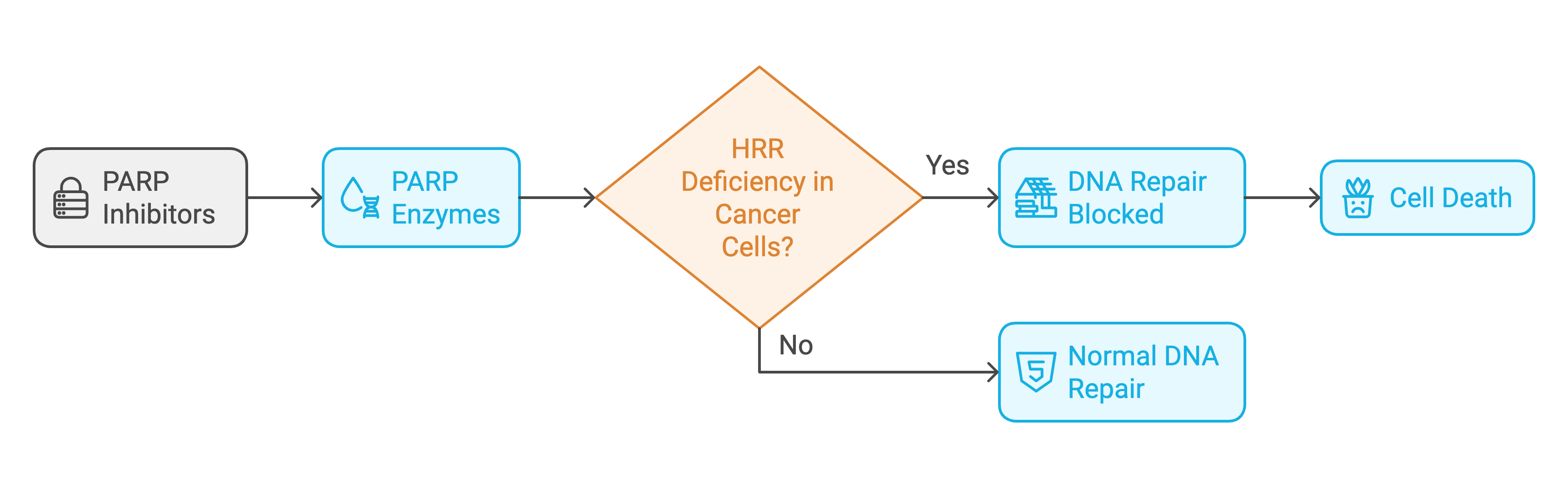
Polyadenosine diphosphate - ADP -ribose - polymerase (PARP) is a cellular enzyme that helps repair single-strand DNA breaks. PARP enzymes repair these single-strand DNA breaks in a process called PARylation.
PARP inhibitors block PARylation, preventing the binding of repair proteins. In HRR-deficient prostate cancer cells, the unrepaired DNA breaks that result from treatment with PARP inhibitors cause cell death.
This process is "synthetic lethality" - two conditions that would by themselves not cause cell death but, when present together, cause lethal injury to the cell.
Analogy of how PARP inhibitors work
PARP inhibitors are like wrenches that jam up a specific repair crew in cancer cells responsible for fixing broken DNA. DNA is like a long zipper that contains instructions for how cells work. Sometimes, this zipper can break, a normal part of life. Cells have special repair crews that fix these breaks to keep everything working correctly.
One of these repair crews is called PARP. It's really good at fixing small breaks, like a single tooth missing from our DNA zipper. But when there are bigger breaks, like a whole section of the zipper ripped apart, another crew called the HRR team steps in. This HRR team is like an expert tailor—they can perfectly stitch the DNA zipper back together.
Imagine some cancer cells have a problem with their HRR team—like the expert tailor is out sick. These cancer cells are in trouble because they can't fix big DNA breaks effectively. This problem with the HRR team occurs in cells with mutations like BRCA1 or BRCA2. These mutations disrupt the HRR team, leaving the cancer cells vulnerable.
This is where PARP inhibitors come in to take advantage of the cancer cell’s vulnerability. They block the PARP repair crew, preventing it from fixing small breaks in DNA. In normal cells with a functional HRR team, this isn't a big problem—the expert tailor can still handle the big breaks.
However, blocking PARP is catastrophic in cancer cells with HRR mutations like BRCA1 or BRCA2 and a broken HRR team. The small breaks that can't be fixed turn into big breaks, and the cancer cell can't survive.
That's why men with prostate cancer that have HRR mutations like BRCA1 or BRCA2 are responsive to PARP inhibitors. When the expert tailor is unavailable, removing the only repair crew dooms the cell!
The importance of genetic testing in prostate cancer
Genetic testing plays a pivotal role in the management of metastatic prostate cancer. This testing is particularly critical for identifying homologous recombination repair (HRR) mutations, which can predict responses to therapies like PARP inhibitors
Germline Testing (blood or saliva): Identifies potential inherited cellular mutations.
In one study, 1.8 percent of men with metastatic prostate cancer carried a germline pathogenic DNA damage repair gene. The most common were:
BRCA2 (5.3 percent)
CHEK2 (1.9 percent)
ATM (1.6 percent)
BRCA1 (1 percent)
Somatic Testing (tumor or circulating tumor DNA): Detects mutations specific to cancer cells, including somatic alterations that are not present in germline DNA.
In one study, somatic testing of 3476 prostate cancer tissue samples showed that 23 percent had potentially actionable HHR gene mutations.
Optimal approach to genetic testing
Doctors might miss nearly half of BRCA1 or BRCA2 mutations with germline-only testing. Tumor-only testing may miss pathogenic germline mutations.
Combining germline and somatic testing reduces the chance of missing actionable HRR mutations like BRCA1 or BRCA2.
Prostate cancer is tricky!
Even without inheriting a BRCA1 or BRCA2 mutation, a man’s prostate cancer cells can still mutate and form BRCA1 or BRCA2 mutations. Thus, a doctor might miss the actionable BRCA1 or BRCA2 mutation if they only performed a germline test.
NCCN guidelines for genetic testing in prostate cancer
National Comprehensive Cancer Network (NCCN) guidelines recommend somatic tumor testing for deficiencies in homologous recombination repair (HRR) genes, such as BRCA1, BRCA2, ATM, PALB2, FANCA, RAD51D, CHEK2, and CDK12, in patients with metastatic prostate cancer.
The guidelines also recommend considering testing for HRR mutations in patients with localized prostate cancer that has spread beyond the prostate gland to nearby tissues or lymph nodes but has not reached distant parts of the body.
Of all of the HRR genes involving DNA damage response pathways in prostate cancer, BRCA2 mutations show the most significant response to PARP inhibitors.
The guidelines also recommend:
Tumor testing for MSI-H or dMMR in patients with metastatic castration-resistant prostate cancer (mCRPC).
Considering testing for MSI-H or dMMR mutations in patients with regional or metastatic castration-sensitive prostate cancer.
And considering TMB testing in patients with mCRPC.
I discussed MSI-H, dMMR, and TMB mutations in the last newsletter.
Caveats concerning somatic gene testing
Somatic gene testing requires tumor tissue, such as the prostate gland or a metastatic lesion. If somatic testing occurs later in the course of the disease, it is optimal to biopsy a current metastatic lesion, such as a lymph node or bone. This is because mutations change over time.
Doctors can also order somatic gene testing on a blood sample with a plasma circulating tumor (ctDNA) assay if testing a metastatic lesion is not an option. However, ctDNA assays may miss HRR deletions unless the disease burden is high.
Germline testing is highly accurate, and next-generation sequencing (NGS) has a sensitivity and specificity above 99% for detecting mutations in targeted genes. On the other hand, somatic testing's accuracy is highly variable.
Somatic testing is not as accurate as germline testing because:
A single biopsy might not represent all the genetic mutations of the cancer.
The portion of the tumor sampled during a biopsy may not include all mutations.
If the tumor content in the sample is low, it reduces the sensitivity of the test to detect mutations. This is common when biopsying a metastatic lesion in bone.
Somatic testing may detect mutations that don't drive the cancer but are present due to random genomic instability.
Regardless, it's essential to attempt both germline and somatic testing in metastatic prostate cancer.
Doctors at prostate cancer centers of excellence know how:
to biopsy metastatic lesions
how to interpret germline and somatic test reports
and will likely call the lab if test results need clarification.
One example of when a doctor might need to call the lab about test results is to clarify if a BRCA1 mutation is altered by one gene (monoallelic) or altered by two genes (biallelic). Biallelic alteration of BRCA1 mutations are more likely to respond to PARP inhibitors.
Effectiveness of PARP inhibitors
Several PARP inhibitors are FDA-approved based on clinical trials in men with metastatic castrate-resistant prostate cancer (mCRPC).
Keywords:
Progression-free survival (PFS): The length of time a person with cancer lives without the disease getting worse.
Median overall survival (mOS): The time point after starting treatment when exactly half of the patients in a clinical trial are still alive and half have passed away.
Overall response rate (ORR): The percentage of people in a study whose disease gets smaller or goes away because of a treatment.
Metastatic castrate-resistant prostate cancer (mCRPC): Prostate cancer that has progressed despite androgen deprivation with testosterone levels below 50 ng/dL.
Olaparib (Lynparza)
The U.S. Food and Drug Administration (FDA) approved olaparib in men with mCRPC:
who have disease progression following treatment with an androgen receptor pathway inhibitor (ARPI) like enzalutamide (Xtandi) or abiraterone (Zytiga).
and have a germline or somatic pathogenic HRR gene mutation.
PROfound study
Median overall survival in men with BRCA1, BRCA2, and ATM mutations was 19.1 months in the olaparib group versus 14.7 months in the control group.
Olaparib improved progression-free survival (PFS) by 7.4 months with olaparib versus 3.6 months with androgen receptor pathway inhibitors.
The overall response rate (ORR) was 33% in the olaparib group versus 2% in the control group.
PROPEL study
Olaparib, approved in combination with abiraterone (Zytiga) for men with BRCA1 and BRCA2 mutations, extends PFS to 25 months versus 17 months with abiraterone (Zytiga) alone.
BRCAAWAY study
Olaparib, approved in combination with abiraterone (Zytiga) for men with BRCA1, BRCA2, and ATM mutations, extends PFS 39 months versus 8.4 months with abiraterone (Zytiga) alone.
Rucaparib (Rubraca)
FDA-approved for men with mCRPC:
with BRCA1 or BRCA2 mutations
after having received taxane chemotherapy with Docetaxel (Taxotere) or Cabazitaxel (Jevtana).
TRITON2 study
Rucaparib showed a 44% response rate in men with BRCA1 and BRCA2 mutations (no control group for comparison).
TRITON3 study
Rucaparib showed a PFS of 11.2 months in men with BRCA1 and BRCA2 mutations versus 6.4 months in the control group.
Niraparib and abiraterone (Akeega)
FDA-approved niraparib in combination with abiraterone for men with mCRPC with BRCA1 and BRCA2 mutations.
MAGNITUDE study
Niraparib plus abiraterone showed a PFS of 19.5 months in men with BRCA1 or BRCA2 mutations versus 10.9 months in the control group.
Talazoparib (Talzeena)
FDA-approved in combination with enzalutamide:
in men with mCRPC
and any of the following HRR gene mutations: ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, or RAD51C.
TALAPRO-1 study
Talazoparib plus enzalutamide showed an overall response rate (ORR) of 29.8%, the highest in BRCA1 and BRCA2-mutated patients
TALAPRO-2 study
Radiographic Progression-Free Survival (rPFS)
HRR-Deficient Population
Treatment arm (talazoparib + enzalutamide): 30.7 months
Control arm (talazoparib + enzalutamide): 12.3 months
Median Overall Survival (mOS)
HRR-Deficient Population
Treatment arm (talazoparib + enzalutamide): 45.1 months
Control arm (talazoparib + enzalutamide): 31.1 months
Non-HRR Population
Treatment arm (talazoparib + enzalutamide): 46.6 months
Control arm (talazoparib + enzalutamide): 37.4 months
“TALAPRO-2 is the first PARP inhibitor plus [androgen receptor pathway inhibitor (ARPI)] combination study to show not only a statistically significant, but also a clinically meaningful improvement in overall survival in patients with metastatic CRPC in unselected and in HRR-deficient [patients],” Neeraj Agarwal, MD, FASCO, Huntsman Cancer Institute at the University of Utah, Salt Lake City, UT
Risks associated with PARP inhibitors
Potential side effects of PARP inhibitors include:
The lowering of white blood cells, red blood cells, and platelets.
Nausea, vomiting, diarrhea, constipation and abdominal pain.
Fatigue, weakness, cough, shortness of breath, and abnormal liver enzymes.
Blood clots in the lungs or legs, especially with olaparib.
Potential long-term toxicity of PARP inhibitors includes:
Myelodysplastic syndrome - a type of blood cancer where your bone marrow doesn't make blood cells properly.
Acute myeloid leukemia - a type of blood cancer where the bone marrow makes too many broken white blood cells that don't work properly.
Researchers are exploring ways to mitigate these risks, including using intermittent dosing.
What you can do
Given the nuanced decision-making involved in genetic testing and the use of PARP inhibitors, it's critical to seek care at a prostate cancer center of excellence. These centers have the expertise to order and interpret genetic tests and personalize treatment strategies effectively. They also know how to properly prescribe PARP inhibitors and change the dosing if side effects occur.
I apologize that the last two newsletters are so science-heavy. I promise to lighten up on the next one:-))
Until the next newsletter, stay healthy.
Much love,
Keith