
False-positive Axumin PET Scan - 021
One reason why second opinions are important

In the last newsletter, I mentioned I'd had an incorrectly interpreted Axumin positron emission tomography (PET) scan in April 2021. That type of PET scan uses a radiolabeled synthetic L-leucine amino acid. Rapidly dividing prostate cancer cells preferentially take up this amino acid compared to normal cells.
Besides this amino acid uptake in prostate cancer cells, there are differing degrees of normal uptake in healthy tissues, including the liver, bone marrow, lung, heart, pancreas, pituitary and salivary glands, bowel, and muscles. A lesion suspected to be cancerous lights up brighter than the bone marrow or blood pool.
I'd had an Axumin scan three years prior, which showed no evidence of cancer. The April 2021 PET scan's interpretation was different. It read,
"Focal increased uptake in or adjacent to the anterior wall of the rectum and the prostate bed as described above. Worrisome for recurrent tumor."
False-positive
When Dr. Stroud, my current radiation oncologist, took over my care, I asked him why the April 2021 PET scan showed uptake in the prostate bed when none of my other PET contrasted tomography (CT) or magnetic resonance imaging (MRI) scans after it showed a tumor in that area.
All of the PET scans I've had since that Axumin PET scan have been prostate-specific membrane antigen (PSMA) PET scans, which light up in areas where prostate cancer cells accumulate a protein called PSMA. PSMA PET scans are considered more accurate than Axumin PET scans. This literature review concluded that "PSMA was able to detect a greater number of lesions than Axumin in patients that had undergone both scans."
Remembering how heterogenous, or diverse, prostate cancers are, if there was a tumor in my prostate bed that didn't contain PSMA, it might light up on an Axumin scan but not a PSMA scan. So he carefully evaluated the prostate bed and rectal wall in all the scans I've had since that Axumin scan and told me, "there is no evidence of tumor in the rectal wall or prostate bed."
Dr. Stroud said that the radiologist interpreted the brightness of my anal sphincter as tumor tissue. This inaccurate interpretation is what's known as a "false-positive" finding. This review article notes that the "pubococcygeus and anal sphincter muscles show uptake" when using an Axumin scan in men like me who've undergone a prostatectomy.
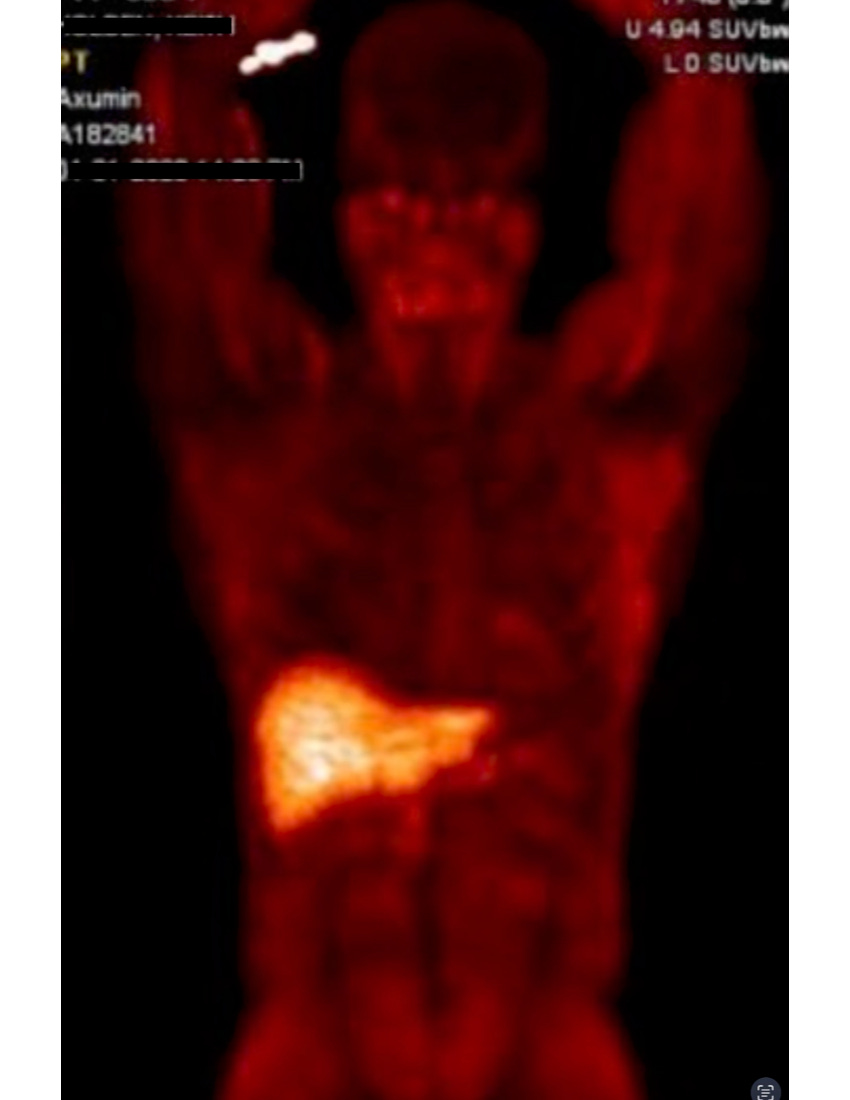
As you can see from the image of my Axumin scan in this article, muscles also uptake the synthetic amino acid. The bright red abdominal muscles reflect this uptake, and the anal sphincter is a tight bundle of muscles. The brightest part of this Axumin scan image is the liver, which has the highest uptake of all.
The accurate interpretation of a PET scan and any other radiologic image is very reader-dependent, meaning it involves subjective interpretation by the person reading the images. So even though my PSA tumor marker at the time was 20, the Axumin scan really didn't show any cancer, which is unusual.
PSMA PET theranostics
When I first started studying PSMA PET scans, I was intrigued by the ability to use these scans as a two-part theranostic approach to treating prostate cancer. Since I was intolerant of testosterone-inhibiting treatments and had already undergone surgery and traditional radiation, I was interested in potentially getting treated with PSMA radioligand therapy (RLT).
Theranostics involving PSMA is a two-part process where first, a diagnostic PSMA PET scan detects tumor cells. In the second part, a therapeutic radioactive ligand (radioligand) is injected and latches onto the PSMA protein on the tumor's cell surface to deliver a precise 1 mm burst of radiation.
Concordance
But I was also naive about how it all worked. I wrongly thought that as long as I had a concordant scan, meaning the findings on my Axumin PET scan matched my PSMA PET scan, I’d be a good candidate for the radioligand treatment. Concordance means that the metastases showing up on the two different PET scans matched; therefore, all metastases had the PSMA protein on their cell surfaces and were vulnerable to this precision radiation.
Standardized uptake value (SUV)
But concordance is only part of the criteria for success in PSMA radioligand therapy (RLT). Researchers are finding you need a higher baseline standardized uptake value (SUV) to increase your chances for a better PSMA radioligand success rate.
SUV is a measure used in positron emission tomography (PET) imaging to assess the uptake of radioactive tracers in tissues, in this case, PSMA. Interpreters read the SUV on the scans as low, intermediate, or high, giving them a specific number on a scale. A high SUV indicates an increased radiotracer uptake, suggesting higher metabolic activity of cancer cells.
My PSMA PET scans have shown low to intermediate SUV uptake in the metastatic lesions in my lymph nodes; therefore, I'm not a good candidate for PSMA RLT therapy. Even if I were a good candidate with a high SUV uptake, I'd have to go to Germany, as only hormone-resistant prostate cancer patients who are on testosterone suppression and have undergone chemotherapy are eligible for RLT in the United States.
Resistance to PSMA radioligand therapy (RLT)
Sadly, studies show that some patients have an inherent resistance to PSMA RLT - 30% in the VISION trial and 17% in the TheraP trial. In addition, researchers believe that most men will eventually develop resistance to this therapy. But like all advanced prostate cancer therapies, it can buy you time. As I've previously mentioned, there is always the chance you'll be an outlier to treatment resulting in a durable remission or cure.
Proton therapy
So based on this information, we decided to use proton therapy to go after the visible metastatic deposits in the lymph node chains on each side of my aorta. We'll soon know whether that decision was correct. In the meantime, I feel that decision was best for me.
In the next newsletter, I'll discuss my proton therapy and some strange and unexpected ways it affected my body and mind. Until then, stay strong and stay positive.
Lots of love,
Keith R. Holden, M.D.