
Lowering Testosterone Increases Heart Attacks and Strokes - 044

The leading cause of death in men in the United States is heart disease. The second leading cause of death in men is cancer, and prostate cancer is the second most common cancer in men.
In 2024, an estimated 299,910 men will be diagnosed with prostate cancer, and 35,250 will die from the disease.
Androgen deprivation therapy
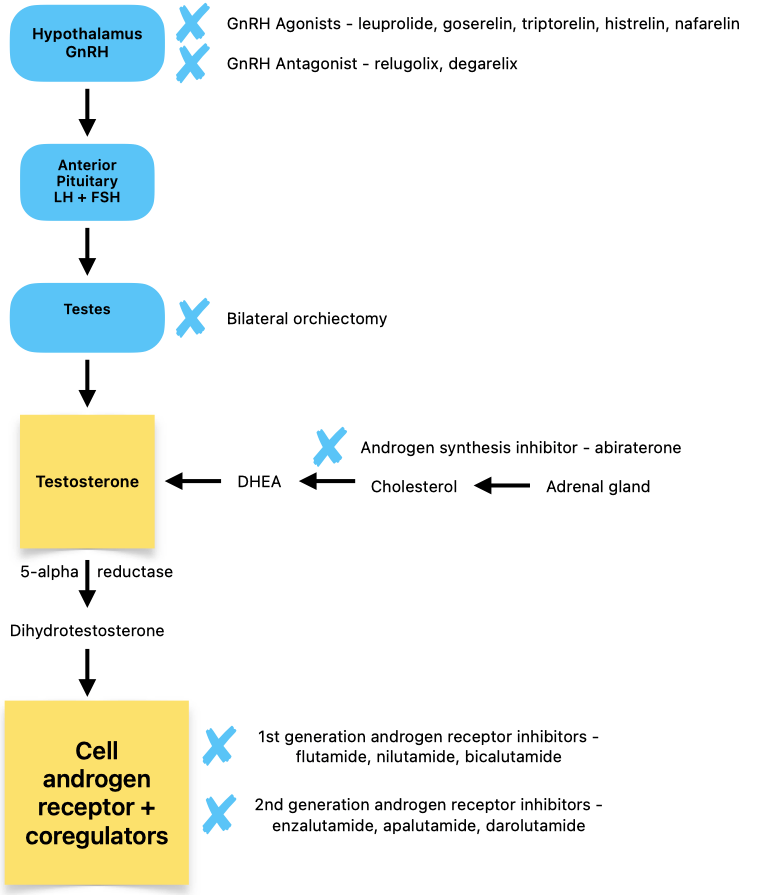
The mainstay therapy for advanced prostate cancer involves either suppressing or blocking the primary androgen testosterone, resulting in androgen deprivation.
Androgen deprivation therapy includes:
Bilateral orchiectomy (removal of testicles)
First-generation androgen receptor inhibitors (oral)
Flutamide( Eulexin) nilutamide (Nilandron), bicalutamide (Casodex)
Second-generation receptor inhibitors (oral)
Enzalutamide (Xtandi), apalutamide (Erleada), darolutamide (Nubeqa)
Gonadotropin-releasing hormone receptor (GnRHR) agonists (injectable)
Leuprolide (Lupron, Eligard), buserelin (Suprefact), gosarelin (Zoladex), triptorelin (Trelstar), histrelin (Vantas), nafarelin (Synarel)
Gonadotropin-releasing hormone receptor (GnRHR) antagonists
oral relugolix (Orgovyx), injectable degarelix (Firmagon)
Androgen synthesis inhibitor (oral)
Abiraterone acetate (Zytiga)
Doctors rarely use bilateral orchiectomy because it is invasive and irreversible. Second-generation androgen receptor inhibitors are preferred over first-generation androgen receptor inhibitors because they bind better to the androgen receptor and result in higher overall survival.
Guidelines for advanced prostate cancer recommend combining gonadotropin-releasing hormone receptor agonists or antagonists with either second-generation androgen receptor inhibitors or with abiraterone acetate.
Abiraterone acetate appears to have the highest cardiovascular risk
The downside of choosing abiraterone acetate is that patients must take it with 5mg of prednisone daily. Because abiraterone blocks the production of cortisol from the adrenal glands, they must take prednisone to replace the lost cortisol and mitigate other potential side effects.
Even low-dose prednisone, when taken long-term, has a slew of dangerous potential side effects, including:
Elevated blood pressure
Swelling
Changes in blood sugar
Increased appetite and weight gain
Insomnia
Osteoporosis (thinning of bones)
Mood changes
Bruising and skin thinning
In a meta-analysis, abiraterone acetate was the only drug shown to increase the risk of cardiovascular events in both observational studies and randomized controlled clinical trials.
In an observational study of over 6000 patients with metastatic prostate cancer, “compared to enzalutamide, abiraterone was associated with a 31% increased risk for MI (myocardial infarction) or stroke.”
Gonadotropin-releasing hormone receptor (GnRHR) agonists versus antagonists
GnRHR agonists, which are all long-acting injectable drugs, are less expensive than the GnRHR antagonist oral relugolix. The injectable GnRH antagonist, degarelix, is comparable in cost to the GnRHR agonists.
GnRHR agonists turn off testosterone production in a roundabout way by initially increasing testosterone levels followed by a decrease in testosterone. GnRHR antagonists immediately shut off testosterone production, which prevents the initial testosterone surge associated with GnRHR agonists.
In certain instances, the testosterone surge caused by GnRHR agonists can be problematic for men with very advanced disease. A relatively inexpensive way to correct this problem is to give these patients an antiandrogen, such as flutamide, bicalutamide, or nilutamide, about one week before the GnRHR agonist.
Once testosterone levels are castrate, doctors will stop the antiandrogen. You might ask, "Why not give everyone a GnRHR antagonist instead of a GnRHR agonist?" Regarding oral relugolix, the main reason is cost.
This article reported the Average Wholesale Price for a 3-month injection of leuprolide is $1626, while 84 tablets of relugolix cost $8254.
Most men with advanced prostate cancer don't experience complications from "testosterone surge." And for those that might experience complications, the GnRHR antagonist, degarelix is a good option, as long as the patient's insurance covers it. My insurance company would not pay for degarelix.
Androgen deprivation therapy and cardiovascular events
All forms of androgen deprivation therapy increase the risk for cardiovascular events, including:
Sudden cardiac death
Myocardial infarction
Heart failure
Cardiac arrhythmias
Uncontrolled hypertension
Stroke
These increased cardiovascular risks appear highest in men with a history of cardiovascular disease, longer duration of androgen deprivation therapy (ADT), and in men with castrate-resistant prostate cancer.
A meta-analysis showed that "animal and human studies suggest that the mechanisms by which ADT increases CV risk include increased atherosclerosis, dyslipidemia, metabolic syndrome, and insulin resistance."
Do GnRHR antagonists have less cardiovascular risk?
There is some evidence that the gonadotropin-releasing hormone receptor (GnRHR) antagonists - oral relugolix and injectable degarelix - may have less cardiovascular risk than the gonadotropin-releasing hormone receptor (GnRHR) agonists, such as leuprolide.
A study published in the New England Journal of Medicine in 2020 compared oral relugolix and injectable leuprolide and reported that relugolix had "a 54% lower risk of major adverse cardiovascular events than leuprolide."
That may seem like a dramatic reduction in cardiovascular events, but 54% was a relative risk reduction. Relative risk reductions can overstate the magnitude of risk reduction compared to absolute risk reduction. In fact, low major cardiovascular event rates in both groups translated into an absolute risk reduction of only 3.3%.
A systematic review of GnRHR antagonists' cardiovascular events compared with GnRHR agonists published in 2023 determined that "there is insufficient high-quality, randomized evidence to definitively answer the question of whether or not GnRH antagonist therapy is superior to GnRH agonist therapy in terms of CV safety, particularly among those with established CV disease."
A big blow to the idea that GnRHR antagonists have less cardiovascular risk than GnRHR antagonists came when the drug company funding the PRONOUNCE clinical trial stopped it early after it was determined the trial would not achieve its hoped-for effect.
The PRONOUNCE trial compared degarelix to leuprolide, looking at a primary endpoint of cardiovascular events in prostate cancer patients who were at high risk for cardiovascular events. Sponsors did a futility analysis and found that both groups had an equal number of cardiovascular events - 5% - and that continuing the study would not change that finding.
Interestingly, a cardiologist evaluated all men in the study as part of clinical trial criteria, and intensive cardiovascular risk management appears to have erased any benefit of GnRHR antagonists over agonists.
Intensive cardiovascular risk management
Considerations for all men prescribed ADT for prostate cancer:
They should be made aware of potential cardiovascular complications associated with ADT.
Assess for cardiovascular risk and refer them to a cardiologist if they have multiple risk factors or a previous cardiovascular event.
Care teams should monitor blood pressure and for signs and symptoms of cardiovascular disease at each visit.
In addition, these men should be encouraged to follow and monitor the American Heart Association's Life's Essential 8:
(1) eat better, (2) be more active, (3) quit tobacco, (4) get healthy sleep, (5) manage weight, (6) control cholesterol, (7) manage blood sugar, and (8) manage blood pressure.
The future
By now, you all know I’m not a fan of androgen deprivation therapy and have avoided it after a disastrous four months of intolerable side effects in the summer of 2018. I’m a huge advocate for clinical trials that research other treatment options.
Eventually, CRISPR gene-editing therapy will have a major impact on overall survival in advanced prostate cancer. It can’t come soon enough.
Until next time, stay well.
Much love,
Keith